Pre-final practical
75 year female brought in an unconscious state-
I've been given this case to solve, in an attempt to understand the topic of "patient clinical data analysis" to develope my competency in reading and comprehending clinical data - including history, clinical findings, investigations - and come up with diagnosis and treatment plan.
Following is a brief about the case.
CHIEF COMPLAINTS:
A 75 year old female, home-maker by occupation and a resident of Miryalguda was brought to the casualty in an unconscious state.
HISTORY OF PRESENT ILLNESS:
*20 years ago - she had chest pain, palpitations and was diagnosed with MI. Stent was placed.
During pre-op investigations, she was also diagnosed with Diabetes, Hypertension and Asthma for which she is on regular medications.
*2017 -
Patient complained of shortness of breath, drowsiness and pedal edema.
Sleep study was done and obstructive sleep apnea was diagnosed. She was advices to be on BiPAP from then
*December, 2021
She had similar complaints of shortness of breath frequently for which she was treated at home.
Two of these episodes were serious and needed hospital admissions - patient recovered in two days.
*March, 2022.
6:30 am
Patient developed shortness of breath
↓
BP measured - increased to 180/100 mm of Hg
↓
1 dose of Labetalol injection given
↓
Patient stable for 3 hours and then her condition started to deteriorate
↓
10:30 am
Taken to hospital
Given a second dose of Labetalol.
Referred to a hospital in Hyderabad.
↓
11:30 am
Patient and attendent stared for Hyderabad in an ambulance
↓
12:30 pm
BP raised and pulse dropped.
Her heart stopped functioning and she fell unconscious
↓
She was rushed to our hospital immediately
↓
6 rounds of CPR was done and patient was shifted to ICU after revival.
↓
She was then given anesthesia and put on ventilator.
↓
She had a few episodes of abnormal movements
(A few on 29/03/2022 - day of admission and 1 on 30/03/2022)
Note : After 2017 tests, she was advised to be on regular BiPAP.
Note : After 2017 tests, she was advised to be on regular BiPAP.
PAST HISTORY :
* History of
- Diabetes since 5 years - Metformin Tab.
- Hypertension since 5 years - Telmisartan Tab.
- Asthma since 5 years - Ipratropium bromide and Budesonide (nebulised form when needed)
PERSONAL HISTORY:
*Diet - Vegetarian
* Appetite - Normal
* Bowel and Bladder - Regular
* Sleep - Adequate
* Allergy- None
* Addition- None
FAMILY HISTORY:
There is no significant family history.
GENERAL EXAMINATION :
The patient is unconscious.
Well built and nourished.
Pedal edema present - upto the ankle - pitting type.
No- pallor, icterus, clubbing, cyanosis, lymphoedenopathy.


Vitals :
On 30 March 2022 :
*Temperature - 98 degree F
* Pulse - 90 bpm
* Respiratory rate - 18cpm
*BP - 160/90 mm of Hg
* SpO2 - 98(on ventilator) - 35 on admission.
On 31 March 2022 :
Temperature - 102F
Pulse 118 bpm
RR- 12 cpm
BP - 160/80 mmHg
Spo2 - 98(on ventilator)
GRBS - 146 mg/dl
SYSTEMIC EXAMINATION:
* CVS - S1 S2 heard.
* Respiratory System - normal breath sounds heard.
INVESTIGATIONS :
29/03/2022 :
* Hemogram-
HB 8.5
TLC 13,600
PCV 27.4
MCH 26.6
MCHC 31
PLT 2.0
P.S NORMOCYTIC, NORMOCHROMIC with neutrophilic leucocytosis
Serum iron : 45ug/dl
RBS: 211mg/dl
HbA1c : 6.8%
*Liver Function Tests-
TB 0.57
DB 0.16
AST 148
ALT 123
ALP 180
TP 4.7
ALB 2.2
* Renal Function tests :
Blood Urea: 49mg/dl
S. Creatinine: 1.9mg/dl
Na 142
K 4.7
Cl 98
* CUE:
ALB ++
Sugars nil
Pus cells 4-5
Epithelial cells 1-2
*ABG :
ABG post CPR fio2 100%
pH 6.88
PCo2 107
PaO2 77.4
HCO3 1108
SpO2 82.5
Interpretation : Metabolic and respiratory acidosis
ABG day 0 evening fio2 80%
pH 7.46
PCo2 32.8
PaO2 146
HCO3 23.1
SpO2 96.8
ABG day 1 morning fio2 40%
pH 7.4
PCo2 31.9
PaO2 80
HCO3 21.5
SpO2 94.7
*ECG:
Post cpr
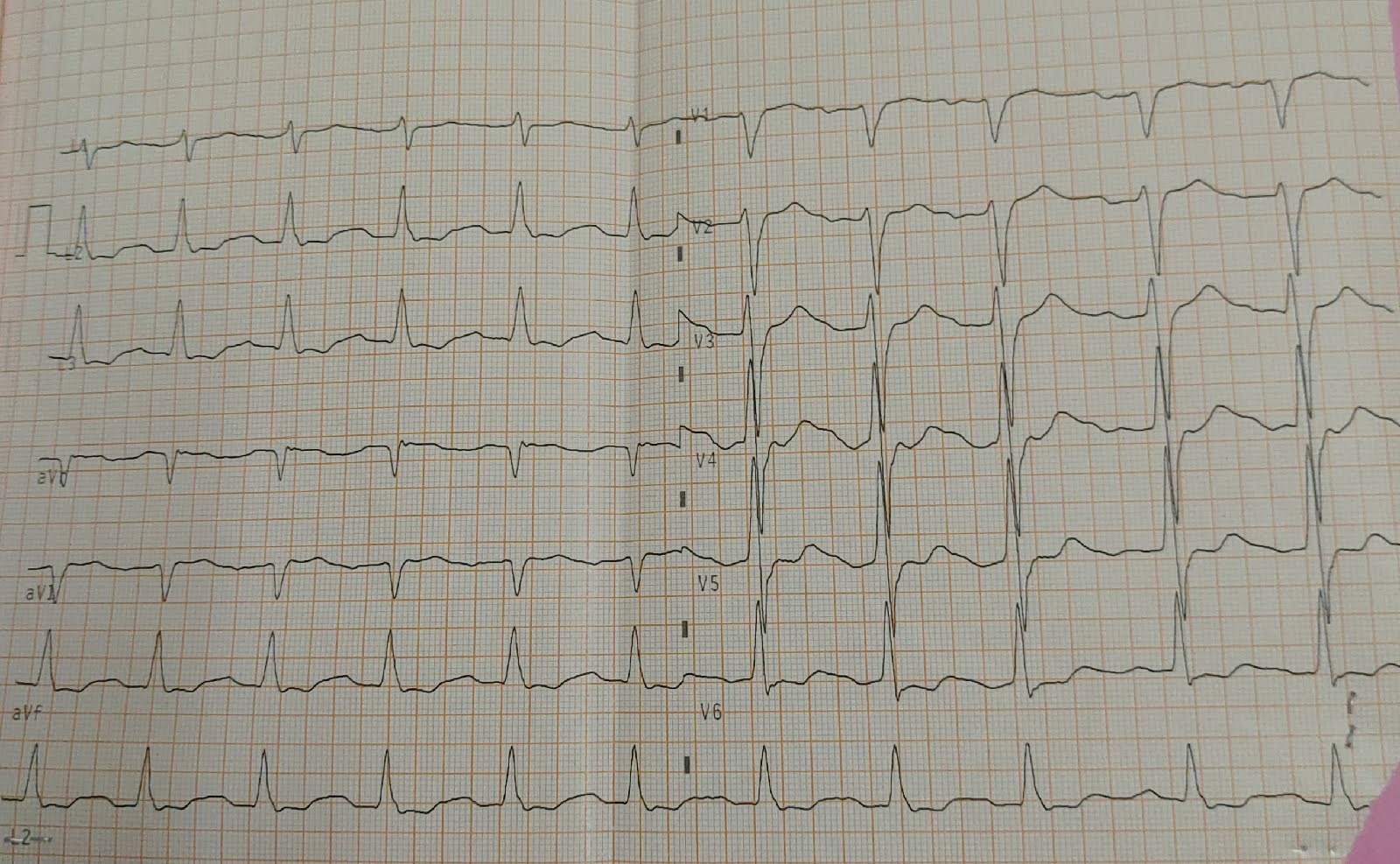
On 30 March

2D echo
Concentric LVH
Sclerotic AV
EF 58%
RVSP 35 mmHg
Diastolic dysfunction +
CXR :
After admission

Cavity in right middle lobe, cardiomegaly present.
On 30 - 03-22 :



*Ventilator settings
PROVISIONAL DIAGNOSIS:
Type 2 respiratory failure with obstructive sleep apnea, came with hypertension and cardiac arrest.
TREATMENT:
*IVF NS/RL @50ML/HR
*Inj. Pan 40 mg IV OD
*Inj. Zofer 4 mg IV SOS
*Inj. Midazolem titrate B/W 0.1 - 3 mg/Kg
*Inj. Atracurium @ 0.8ml/hr (10mcq/hr)
*Inj. Levipil 1gm IV STAT
*Inj. Levipil 500 mg IV TID
*Inj. Clexane 60mg sc OD
*Ryle tube feeds milk+protein 100ml, water 100ml 4hourly.
*Propped up position
*Air bed with position change 2 hourly.



Reference Log - Intern
Case taken with :
Neha T



Comments
Post a Comment